What is Biceps Tendonitis, and What Can YOU Do for it?
If you’re a gym goer you’ve likely heard someone talk about biceps tendonitis or rotator cuff pain. Often times, anytime someone has shoulder pain they either blame the rotator cuff or the biceps tendon, wither that’s the true cause of their shoulder pain or not. So in this blog we aim to address WHAT IS BICEPS TENDONITIS AND WHAT CAN BE DONE FOR IT?
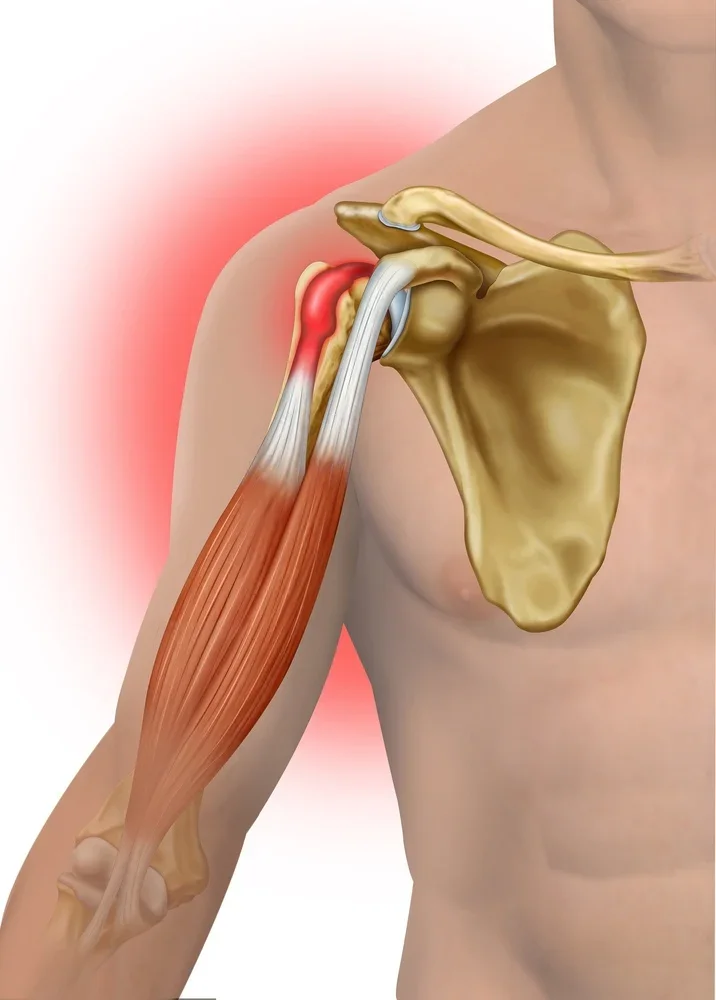
Biceps tendonitis, presents as anterior shoulder pain near the glenoid humeral joint and AC joint, this is where the long head of the biceps tendon originates. To better understand biceps tendonitis or really ANY tendonitis, we need to lay the ground work through a proper understanding on medical terminology. Unfortunately, tendonitis, tendinosis, and tendinopathy are frequently used term and can often be used interchangeably. However, they mean different things and are often used incorrectly!
An -itis, -osis, or -opathy all indicate that something has gone wrong and is not in its normal state, but they DONT mean the same thing. An -opathy indicates a disease, in the case of tendinopathy, it refers to a disease or abnormal state of the tendon and is more broad term. While -itis indicates inflammation, often the result of acute trauma or stress. It is important to remember, inflammation is part of the body’s natural response mechanism and USUALLY, shouldn’t be interfered with as it is often due to micro-tears from the tissue being overladed. In this case -itis means inflammation of the tendon, particularly the biceps tendon. Lastly, -osis, is NOT associated with inflammation, rather, it is associated with chronic or long-term stress of the tissue. In the case of tendinosis, it implies chronic stress of the tendon that has led to degeneration at the cellular and tissue level.
While tendonitis and tendinosis, can be diagnosed through various imaging modalities such as MRI or MSK ultrasound they can also be diagnosed through a detailed physical exam encompassing palpation, muscle testing and special orthopedic tests. In this particular blog we will focus on tendonitis.
Tendonitis in general is within the category of overuse syndromes, plays a key role in conditions such as repetitive stress injuries and occupational overuse. The majority of overuse syndromes involve a inflammatory response. This inflammatory response is provoked by repetitive movements, stress and sustained tension on the tendon or muscle itself.
Again, in the acute stage tendonitis involves inflammatory cells and mediators, however, in the cute state this is NOT associated with degeneration. However, if the stress is not removed, the inflammatory response will lead to tissue breakdown over time, a degenerative process, known as tendinosis.
While we are focusing on the biceps tendon, tendonitis is a common condition affect several tendons throughout our body such as the supraspinatus (RTC), lateral epicondylitis AKA tennis elbow, Achilles tendonitis, etc. etc.
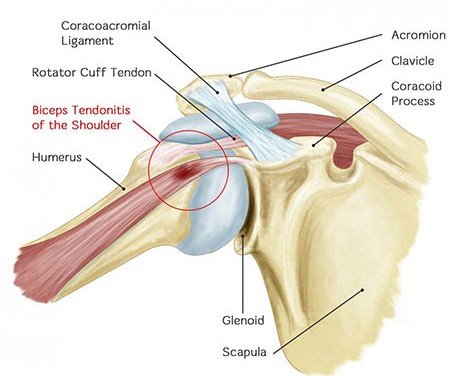
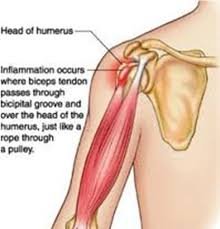
The biceps tendon affects the long head of the biceps tendon and is a common cause of shoulder pain. The long head of the biceps tendon is susceptible to injury because of its positioning along the anterior shoulder as it passes through the bicipital groove and inserts onto the superior aspect of the glenohumeral joint. This position puts it at risk for acute damage caused by impingement of the tendon in the subacromial space. This impingement overtime and in repetition can easily lead to bicipital tendonitis. Another contributing factor in biceps tendonitis is the rotator cuff, and rotator cuff disease can often be a component of impingement syndrome.
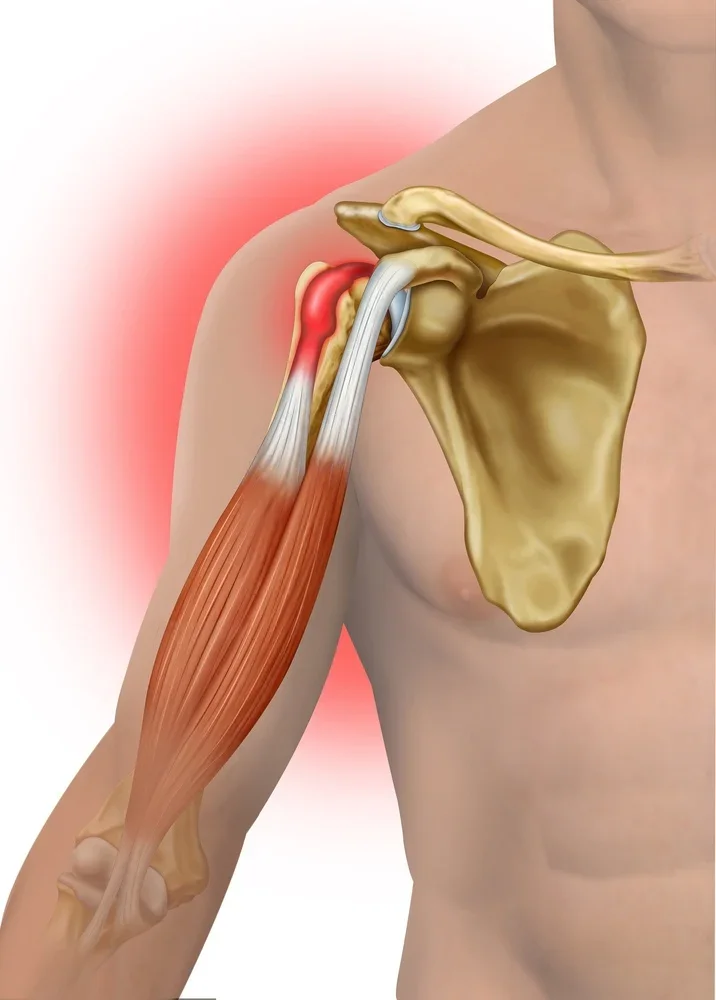
If you’re like me, you may be more of a visual learner, so hear are a few pictures of the shoulder anatomy involving the biceps tendon, then it may be easier to understand how the biceps tendon can become prone to injuries.
Due to its position, in the subacromial space, it is easy to see how overhead activities such as hitting a tennis ball, throwing a ball repetitively or even swimming can lead to irritation of the biceps tendon inciting an inflammatory response. However, biceps tendonitis is not just seen in competitive athletes, but is also commonly seen in the average gym-goer, due to an inability to properly extend the thoracic spine as well as tight pectorals or latissimus musculature, which inhibits proper shoulder girdle mechanics.
While it is often clear to see how overhead athletes are subjected to bicipital tendonitis, it may be less clear in other populations. However, anyone who can’t freely move their arms overhead, is also at risk. Again, referring to the above images, the biceps has two heads or muscle belly’s that originate near the shoulder and then merge into a common insertion tendon, across the elbow at the radius. Thus, the biceps has a functional role at both the shoulder and the elbow! The short head of the biceps tendon, inserts EXTERNAL to the shoulder joint and is therefore, rarely involved in shoulder impingement syndrome. However, the long head of the biceps passes through the bicipital groove of the arm and then makes a 90 degree turn across the head of the humerus, attaching to the superior aspect of the glenoid fossa (socket of the ball and socket shoulder joint). Because of the path of the long head of the biceps it has a key role in both stabilization and movement of the arm.
However, because of its positioning in the subacromial space, optimal movement of the humerus, scapula and clavicle is necessary to protect the muscles and tendons of the upper arm. Scapulohumeral rhythm is, key and consists of integrated movements of the glenohumeral joint, scapulothoracic, AC joint, and SC joints. These joints should work in a rhythmic fashion during shoulder and upper arm movements. When they work properly the coordinated movements function to :
Allow for full range of motion
Maintain optimal contact between the head of the humerus and the glenoid fossa, improving joint stability
Maintain optimal length-tension relationships for improved stability, force production and force reduction
While we won’t go into a detailed shoulder evaluation in this blog, identifying imbalances or improper mechanics of the shoulder girdle is key to properly rehabbing or even preventing shoulder dysfunction such as bicipital tendonitis. Various muscles that are not necessarily thought of as shoulder muscles act on the scapula and can inhibit proper scapular mobility. If the scapula cant move efficiently the shoulder can’t move and function efficiently leading to shoulder pathology such as bicipital tendonitis.
Below, we will provide some stretches and corrective exercises aimed at restoring proper shoulder gridle mechanics.
Inhibit-Self myofasical release
Latissimus dorsi: Get into a side-lying position with the foam roller positioned toward the bottom of the shoulder blade. Slowly roll all way up to the armpit and the back of the shoulder joint.
2. Posterior capsule: Position a massage ball just behind the shoulder joint, on the rear deltoid.
3. Thoracic spine: In a supine position, slowly roll the length of the thoracic spine. Perform shoulder flexion motions to encourage thoracic extension.
Lengthen - Static Stretching
Latissimus dorsi: Take to the first point of tension and hold for 30-45 seconds.
2. Sleeper Stretch: Side-lying with the arm abducted to 90 degrees and shoulders stacked, slowly internally rotate arm with opposite hand and hold for 30-45 seconds.
3. Thoracic Extension: In a supine position with a foam roller positioned mid-thoracic spine and hands supporting the head, slowly lean back to the first point of tension. DO NOT let bottom ribs flare up as this indicates the lumbar spine is beginning to extend.
Activation
Shoulder Y’s: Lay prone over an exercise ball with your elbows straight and arms out in front of your body as shown (Y’s). The shoulder should be approximately 120 degrees abducted. Slowly raise your arms upward and return to original position. Your thumbs should be pointed upwards the entire time.
2.
Shoulder T’s: Similar to above, lay prone over an exercise ball with your elbow straight and your arms out to the side (T’s). Slowly raise your arms upward and return to original position. Your thumbs should be pointed upwards the entire time, or you may also add light weights.
3. Shoulder internal rotation: With the elbow flexed to 90 degrees, keep your elbow adducted at your side (can use a towel or small ball). Use either bands or cable machine, keeping your elbow at your side bring your fist across your chest, resulting in internal rotation of the shoulder.
4. Shoulder external rotation: With the elbow flexed to 90 degrees, keep your elbow adducted at your side (can use a towel or small ball). Using either bands or cable machine, keeping your elbow at your side bring your fist away from your chest, so your fist is in plane to your truck.
We hope this blog provides your with a better understanding of shoulder dysfunction, particularly bicipital tendonitis. If you are experiencing shoulder pain, come see us for a full evaluation!
Book now!